

Non-syndromic cleft palate or cleft lip/palate
With non-syndromic cleft palate, the palate is partially or completely open, but no other congenital anomalies are present.
This condition affects swallowing, eating and speech. Children have a higher risk of external ear infections.
Surgical repair is indicated; timing of surgery varies between the cleft teams world wide.
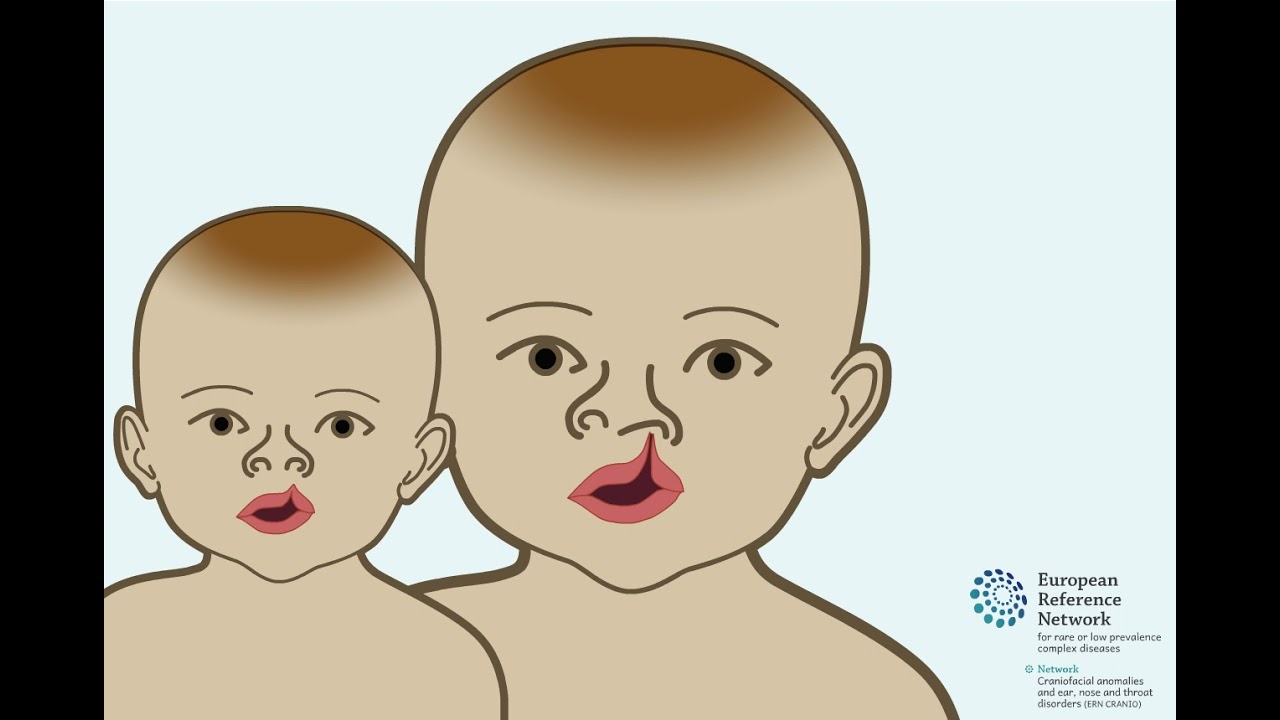
With non-syndromic cleft lip/palate, the lip and palate are involved in the cleft, but no other congenital anomalies are present.
The cleft of the lip can be unilateral (1-sided) or bilateral (two-side). The cleft can be complete (involving the nasal floor) or incomplete.
If the clefting involves the alveolar ridge, a notch or true cleft can be seen on one or both sides. Additionally, the palate can be partially of completely open. Surgical repair is indicated; the timing and stages in which this is performed differ between cleft teams.
Syndromic cleft palate or cleft lip/palate
With syndromic cleft palate, the palate is partially or completely open, and other congenital anomalies are present.
The cleft palate affects swallowing, eating and speech, but these factors can also be hampered by the underlying syndrome.
With syndromic cleft lip/palate, the lip and palate are partially or completely open, and other congenital anomalies are present. The cleft lip/palate affects swallowing, eating and speech, but these factors can also be hampered by the underlying syndrome.
ERN CRANIO endorses the Dutch guideline for 'schisis' [the term 'schisis' in Dutch encompasses all types of facial clefts, most commonly clefts of the lip and/or palate].
Informative videos on cleft lip and/or palate
Informative videos on cleft lip and/or palate

Alveolar bone grafting: for children with a cleft lip and/or palate
Embryonic development: Cleft lip and/or palate

Speech surgery: Buccal flap

Closure of a cleft palate
Robin Sequence
The diagnosis Robin sequence is made in case of:
A hypoplasia of the mandible
Breathing difficulties, particularly when sleeping on the back
Glossoptosis
Usually, there is also a cleft palate present.
A distinction is made between isolated and syndromic Robin sequence, depending on the absence of presence of other congenital anomalies. An example of a syndromic Robin sequence is Treacher Collins syndrome.
The breathing disorders in non-syndromic Robin sequence can often be overcome by having the baby sleep on the side or in supine position (combined with a saturation device for monitoring). For syndromic disorders, this should always be attempted, but additional measure may be required.
Disorders with cleft lip/palate as important feature
Facial dysostosis describes a set of clinically and etiologically heterogeneous congenital craniofacial anomalies. These disorders arise as a consequence of abnormal development of the first and second pharyngeal arches and their derivatives during embryogenesis.
These disorders are highly related to breathing problems, and the newborn child should be screened with a sleep study. In general, the major site of obstruction is at the tongue base level. Whenever a child also has a cleft palate, surgical closure of the palate can worsen the breathing problems significantly. Before performing this surgical procedure, one has to be certain that breathing will not become obstructed. This can be done by performing an overnight sleep study with the child wearing a palatal plate that mimics a closed palate.
Breathing problems tend not to lessen with time in facial dysostosis, but need treatment. This can be either supportive measures such as oxygen during the night or CPAP, but it could also require surgical interventions like tracheostoma for severe obstructed breathing and mandibular distraction.
Treacher Collins
Symmetric facial anomalies: Hypoplasia of infraorbital rim and zygomatic arch, coloboma of eyelids, low position of lateral canthi, entropion, microtia, deafness, hypoplasia of mandible, breathing- and feeding difficulties. Often co-occurrence of a cleft palate.
Nager syndrome
Similar to Treacher Collins syndrome, combined with hypoplasia of the thumbs.
Miller syndrome
The facial features are similar to Treacher Collins syndrome.
Burn-McKeown
Symmetric of asymmetric facial anomalies, choanal atresia.